National Research and Innovation Agency, Indonesia.
*Corresponding author: Lucie Widowatic
National Research and Innovation Agency, Indonesia.
Email ID: luci003@brin.go.id
Received: Nov 17, 2025
Accepted: Jan 23, 2026
Published Online: Jan 30, 2026
Journal: Annals of Traditional Chinese Medicine
Copyright: Widowati L et al. © All rights are reserved
Citation: Widowati L. The use of Indonesian medicinal plants by various ethnic groups to treat menstrual disorders within the community. Ann Tradit Chin Med. 2026; 2(1): 1014.
Background: Menstrual disorders, including dysmenorrhea, are characterised by menstrual pain and discomfort experienced by women. In Indonesia, traditional healers (locally known as hattra) commonly use herbal remedies to alleviate dysmenorrhea symptoms. Various medicinal plants used for this purpose have been documented through the 2015 and 2017 Research on Medicinal Plants and Herbal Medicine (Ristoja) surveys conducted by the Indonesian Ministry of Health. Methods: This study further analyses data from Ristoja to provide an overview of the use of medicinal plants for managing dysmenorrhea by traditional healers across different ethnic groups in Indonesia. Results: Scientific evidence supporting the use of medicinal plants for dysmenorrhea was identified through in vitro, in vivo, and clinical studies. A total of 339 herb groups related to menstrual disorders were recorded, originating from 73 Hattra, 77 ethnic groups. Among these, 123 plant species were specifically identified as being used to treat dysmenorrhea. The six most commonly used medicinal plants across different ethnic groups are C. longa, Z. officinale, P. betle, T. indica, L. inermis and C. nardus. Conclusions: Hattra utilises a diverse range of medicinal plants, with several species commonly used across different ethnic groups to treat menstrual disorders. Among these, six medicinal plants have been widely employed and have shown efficacy in in vivo studies. Clinical evidence has been reported for C. longa (turmeric), Z. officinale (ginger), T. indica, and C. nardus. Integrating traditional knowledge with modern scientific research offers significant potential to enhance our understanding of dysmenorrhea and to develop effective natural therapeutic options.
Keywords Indonesia; Traditional herbal medicine; Menstrual disorders.
Dysmenorrhea, or menstrual pain, is a common condition experienced by women worldwide. It is frequently accompanied by symptoms such as nausea, vomiting, diarrhea, headaches, fatigue, and, in some cases, may contribute to depressive symptoms. Menstruation itself is considered an inflammatory process, involving leukocyte infiltration and the release of various inflammatory mediators [1,2].
The condition is primarily attributed to the excessive production of uterine prostaglandins particularly Prostaglandin F2 Alpha (PGF2α) and Prostaglandin F2 (PGF2), which induce inflammation and amplify uterine contractions. Elevated levels of these prostaglandins result in increased uterine tone and highamplitude contractions, ultimately causing pain [3]. Dysmenorrhea has a high global prevalence, with rates varying by region. In Sweden, approximately 72% of women report experiencing menstrual pain, while in the United States, the prevalence reaches up to 90%, with 10–15% experiencing severe symptoms [4]. A study in Kuwait found a oneyear prevalence of 85.6%, with 26% of affected individuals seeking outpatient care and 4.1% requiring hospitalisation due to menstrual pain [5]. In Indonesia, the Ministry of Health reported that around 55% of adolescent girls suffer from dysmenorrhea [6].
Dysmenorrhea can be addressed through both pharmacological and nonpharmacological strategies. Conventional pharmacological treatments typically involve the use of Nonsteroidal Anti-inflammatory Drugs (NSAIDs) and hormonal contraceptives, especially those that act by inhibiting prostaglandin synthesis to alleviate menstrual pain. However, prolonged use of these medications has been linked to adverse effects, including kidney dysfunction, gastrointestinal disturbances, and cardiovascular complications. Furthermore, many adolescents rely on pain relievers and hormonal therapies without sufficient knowledge of these potential risks [7].
In light of these concerns, there has been a rising interest in Complementary and Alternative Medicine (CAM), including herbal therapies, dietary adjustments, and physical modalities. Medicinal plants such as fennel, ginger, and cinnamon, renowned for their antinociceptive (pain-relieving) effects, have been widely employed by practitioners around the world [8,9].
Empirically utilised medicinal plants, which have been traditionally passed down through generations, possess notable therapeutic potential and are generally regarded as safe when used appropriately. These herbs deserve further scientific research to support the development of standardised herbal pharmaceutical products.
In Indonesia, the use of medicinal plants is strongly embedded in cultural traditions and is supported by the country’s abundant biodiversity. Hattra commonly offers herbal treatments based on empirical knowledge inherited through generations. National surveys conducted in 2015 and 2017 (RISTOJA) across all Indonesian provinces documented the widespread use of medicinal plants among Hattra and emphasised the rich cultural heritage of traditional health practices in the country [10,11].
This study aims to explore herbal preparations traditionally used by Hattra in managing menstrual disorders. According to Hattra, these disorders include a range of conditions such as menstrual pain (dysmenorrhea), heavy or scanty bleeding, prolonged menstruation, irregular cycles, and premenopausal symptoms.
This study utilised data from the Research on the Exploration of Local Knowledge of Ethnomedicine and Medicinal Plants Based on Community Participation in Indonesia (Riset Penggalian Pengetahuan Lokal Etnomedisin dan Tumbuhan Obat Berbasis Partisipasi Masyarakat – RISTOJA), conducted by the National Institute of Health Research and Development, Ministry of Health of the Republic of Indonesia (Badan Litbangkes Kemenkes RI) in the years 2015 and 2017.
The 2015 survey was conducted in 125 districts across 24 provinces, involving 96 ethnic groups. In 2017, the study expanded to 65 districts in 11 provinces, covering 100 ethnic groups.
Informants were individuals recognized by their communities for their expertise in traditional healing and the use of medicinal plants. They were selected through purposive sampling, based on recommendations from indigenous leaders, village heads, local health centres, or district health offices.
Data collection employed a combination of structured and open-ended interviews to ensure both the breadth and depth of information obtained. Each research team comprised five members from multidisciplinary backgrounds, including experts in botany (biology, agriculture, forestry), anthropology (anthropology, sociology), and health sciences (medicine, pharmacy, public health, and nursing). The information gathered included demographic data, as well as detailed descriptions of the types and parts of medicinal plants used. This research received ethical approval with clearance numbers LB.02.01/5.2/KE.318/2015 and LB.02.01/2/KE.107/2017.
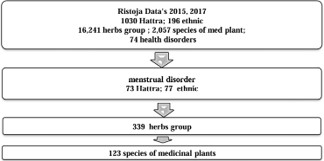
The selection of medicinal plants for menstrual disorders is derived from the documented use of herbal remedies by 73 Hattra and 77 ethnic groups.
| No. | Scientific name | Number of repeatedly concotion | % Contribution to the total number of concotion (N=132) | % Contribution to the Total Number of Med. plants (N=123) | % Contribution to the Total Number of Etnics (N=77) | Island | Ethnic |
|---|---|---|---|---|---|---|---|
| 1. | Curcuma longa L. | 19 | 14,4 | 15,4 | 23,4* | Sumatera | Abung, Daya, Mandailing, Melayu Natuna |
| Jawa | Baduy, Banten, Samin, | ||||||
| Kalimantan | Belangin, Kayung, | ||||||
| Sulawesi | Padoe, Balesang | ||||||
| Nusa Tenggara | Kore, Ende, Mela | ||||||
| Maluku | Roman, Gebe, Kao Dalam, | ||||||
| Papua | Lani | ||||||
| 2. | Zingiber officinale Roscoe | 6 | 4,5 | 4,9 | 7,8* | Jawa | Samin |
| Kalimantan | Galik, Kayanat | ||||||
| Nusa Tenggara | Dompu, Ende, Kore | ||||||
| 3. | Lawsonia inermis L. | 5 | 3,8 | 4,1 | 5,2* | Sumatera | Melayu Batu Bara |
| Jawa | Bawean, Madura | ||||||
| Sulawesi | Bolaang Itang | ||||||
| 4. | Piper betle L. | 5 | 3,8 | 4,1 | 6,5* | Sumatera | Abung, Duano, Pak-Pak |
| Nusa Tenggara | Kore* | ||||||
| Maluku | Roman | ||||||
| 5. | Tamarindus indica L. | 5 | 3,8 | 4,1 | 5,2* | Sumatera | Pegagan |
| Sulawesi | Bonerate | ||||||
| Nusa Tenggara | Ende, Mela | ||||||
| 6. | Andrographis paniculata (Burm. F.) Ness | 4 | 3,0 | 3,3 | 3,9 | Jawa | Jawa |
| Sulawesi | Lalaeo | ||||||
| Nusa Tenggara | Ende | ||||||
| 7. | Cymbopogon nardus (L.) Rendle | 4 | 3,0 | 3,3 | 5,2* | Sumatera | Melayu Natuna, Meranjat, Pak Pak, Peminggir |
| 8. | Graptophyllum pictum (L.) Griff. | 4 | 3,0 | 3,3 | 3,9 | Sumatera | Melayu Natuna |
| Kalimantan | Sanggau | ||||||
| Papua | Galela |

The selected medicinal plants were those used repeatedly in five or more concoctions. Curcuma longa was found in 19 concoctions, Zingiber officinale in six, Lawsonia inermis, Piper betle, and Tamarindus indica in five each. Additionally, three medicinal plants were used in four formulations, six plants appeared in three formulations, 23 plants were found in two formulations, and 86 medicinal plants were reported in only one formulation. Table 1 presents Medicinal Plants Used in Herbal Concoctions for Menstrual Disorders by Traditional Healers Across Various Ethnic Groups in Indonesia.
The sequence of medicinal plants most commonly used for dysmenorrhea, each with a usage frequency greater than 5%, is, in descending order: Curcuma longa, Zingiber officinale, Piper betle, Lawsonia inermis, Tamarindus indica, and Cymbopogon nardus. Scientific evidence supporting the selection of medicinal plants for treating menstrual disorders is based on empirical usage, as well as research findings on their analgesic and antiinflammatory activities demonstrated through in vitro studies, in vivo experiments, and clinical trials involving humans.
Curcuma longa L.
Curcuma longa L., belonging to the Zingiberaceae family, is the most extensively utilised medicinal plant by Hattra (traditional healers) in Indonesia for managing menstrual disorders. Traditionally, it is believed to be effective in alleviating dysmenorrhea. Empirically, C. longa has also been used to address various health conditions such as rheumatism, dermatological issues, constipation, anemia, abdominal cramps, vaginal discharge, influenza, and infections. From a pharmacological perspective, C. longa possesses a broad spectrum of biological activities, including antiinflammatory, antioxidant, hepatoprotective, neuroprotective, chemopreventive, anticancer, antiallergic, and antifungal properties. It also has demonstrated therapeutic potential in treating respiratory and digestive disorders, as well as antihyperglycemic effects. The main bioactive constituents responsible for these effects include curcuminoids, glycosides, terpenoids, and flavonoids [12].
Ethanolic extracts of C. longa have demonstrated analgesic and antiinflammatory activities in preclinical studies using male Wistar rats [13]. Additionally, the extract was shown to inhibit both neurogenic and inflammatory pain responses in a rodent formalininduced pawlicking test model [14].
Clinical investigations in human subjects further support the therapeutic value of C. longa in managing menstrual pain. A study by Kashani et al.reported that daily administration of curcumin significantly reduced pain severity in women with primary dysmenorrhea compared to a placebo group [15]. Another study by Utami et al, evaluated the efficacy of C. longabased drinks for dysmenorrhea, comparing homemade preparations with formulations developed through research. The study employed a pretest and posttest experimental design [16].
Moreover, a clinical trial conducted by Fanaei et al.assessed the effects of curcumin and placebo over three consecutive menstrual cycles, with each cycle involving 10 days of treatment [17]. Initially, there were no significant differences between the groups in serum BrainDerived Neurotrophic Factor (BDNF) levels or Premenstrual Syndrome (PMS) symptom scores. However, postintervention, the curcumintreated group exhibited a marked increase in BDNF levels and a significant reduction in PMS symptoms, including emotional, behavioral, and physical complaints, when compared to the placebo group.
Zingiber officinale Roscoe
Zingiber officinale Roscoe, or ginger, a member of the Zingiberaceae family, is widely recognised for its medicinal benefits, including its use in managing dysmenorrhea. Traditionally, ginger has been employed to alleviate flatulence, suppress coughs, relieve headaches and various types of pain, stimulate appetite, induce perspiration, combat fungal infections, and treat rheumatism. In Indonesian traditional medicine, ginger is often administered as a decoction 15 grams of ginger are boiled in 400 mL of water until the volume is reduced to 200 mL, and this preparation is consumed over a sixday period (three days before and three days after menstruation) [18]. The therapeutic efficacy of ginger is attributed to its rich phytochemical content, comprising around 400 bioactive compounds. The primary constituents, gingerol and shogaol present in the oleoresin fraction (4–7.5%) have been shown to exert analgesic, antiemetic antipyretic, antitussive, hypotensive, cardiodepressive, mutagenic, and antiinflammatory effects [19].
Preclinical pharmacological research has demonstrated that [6]gingerol significantly reduces pain responses in mice subjected to acetic acidinduced writing and inhibits paw edema in the carrageenan model, supporting its analgesic and antiinflammatory activity (Singh et al., 2010). Mechanistically, ginger exerts effects similar to Nonsteroidal AntiInflammatory Drugs (NSAIDs) by inhibiting prostaglandin synthesis via suppression of Cyclooxygenase1 (COX1) and Cyclooxygenase2 (COX2) [20,21].
Goel & Maurya recommended ginger as one of 19 herbal remedies for menstrual pain [22]. A comprehensive systematic review by Jiao et al. (2022) identified 217 plant species across 80 families used for menstrual health in 16 countries, with Z. officinale, Foeniculum vulgare, Angelica sinensis, and Rosa graveolens among the most cited [23].
The effectiveness of ginger in treating primary dysmenorrhea has also been confirmed in clinical trials. Gurung et al. (2022) found that administering ginger from the first day of menstruation for three consecutive days significantly alleviated menstrual pain [24].
According to Mirabi et al. (2014), ginger not only reduced the intensity but also the duration of menstrual pain compared to a placebo [25]. Additional studies demonstrated that ginger’s analgesic effects were comparable to those of mefenamic acid and ibuprofen [26] and it was found to be superior to placebo in reducing pain severity [27].
Lawsonia inermis L
Lawsonia inermis, commonly referred to as henna, has traditionally been utilized to address a variety of health conditions, including gonorrhea, intestinal amebiasis, headaches, and sore throats, as well as being employed as an abortifacient [23,28].
Conversely, pharmacological evidence suggests that L. inermis possesses notable uterotonic properties, capable of inducing uterine contractions comparable to those triggered by acetylcholine. It has also been observed to extend the estrous cycle and lower progesterone levels, alongside reducing the weights of the ovaries and uterus, findings that imply possible gonadotropic inhibition [29].
In light of these physiological effects, the use of L. inermis in women’s reproductive health requires careful consideration. Its potential abortifacient and anti-ovulatory activities highlight the importance of ensuring that traditional healers do not inadvertently misuse this plant in the treatment of menstrual disorders.
Piper betle L.
Piper betle (betel leaf) has long been used in traditional medicine for its diverse therapeutic benefits, including anti-inflammatory, antiseptic, antibacterial, hemostatic, antitussive, carminative, sialagogue, anthelmintic, antipruritic, and mild sedative effects. Pharmacological studies have confirmed that P. betle exhibits various bioactivities such as antimicrobial, analgesic, hepatoprotective, gastroprotective, and respiratory benefits, as well as efficacy in postpartum care. These effects are largely attributed to its phytochemical constituents, including tannins, flavonoids (such as quercetin), eugenol, hydroxychavicol, and chavibetol [30].
Several investigations have highlighted the plant’s analgesic and anti-inflammatory potential. Preclinical evaluations conducted by Fatin et al. (2023) supported these properties [31]. A study by Venkateswarlu and Devanna (2014) using methanol extracts of P. betle in Swiss albino mice subjected to the acetic acid induced writhing test showed a significant reduction in writhing, indicating analgesic activity [32].
For anti-inflammatory activity, Pradhan et al. (2013) employed both acute (carrageenan and dextran induced paw edema) and chronic (cotton pellet induced granuloma) inflammation models in rats [33]. The crude suspension of P. betle demonstrated anti-inflammatory effects comparable to sodium diclofenac within three hours post administration.
Furthermore, consistent analgesic and anti-inflammatory outcomes were observed across various tests, including hot plate, acetic acid induced writhing, and formalin induced nociception.
These findings support the empirical use of P. betle by traditional practitioners and highlight its potential role as a natural alternative in the management of dysmenorrhea.
Tamarindus indica L.
The leaves of Tamarindus indica (tamarind) have traditionally been used to treat rheumatism, wounds, coughs, and fever. Meanwhile, the fruit is commonly employed to aid digestion, enhance the immune system, reduce fever, and promote wound healing. Pharmacologically, the methanol extract of tamarind leaves has shown significant analgesic activity, contributing to pain relief [34].
Interestingly, tamarind is often combined with turmeric (C. longa) in traditional herbal preparations, particularly for the treatment of dysmenorrhea. According to Mulyani et al.,this combination demonstrates stronger antioxidant activity than turmeric alone. The acidic component of tamarind is believed to enhance the analgesic potential of turmeric, forming the basis for its widespread traditional use [35].
This synergy is supported by research from Wu J et al. (2024) in China, which investigated the effect of C. longa processed with vinegar in a rat model of dysmenorrhea characterized by liver depression and Qi stagnation [36]. The vinegar processed turmeric improved liver function, regulated reproductive hormone levels, reduced pain, and improved blood rheology, all of which contributed to its efficacy in relieving dysmenorrhea symptoms.
While turmeric is among the most extensively used medicinal plants for menstrual pain, clinical trials specifically targeting dysmenorrhea remain limited. However, several clinical studies have evaluated the efficacy of turmeric tamarind combinations. In Indonesia, particularly among the Javanese and Madurese ethnic groups, turmeric tamarind herbal drinks are widely known and traditionally consumed by young women to facilitate menstruation.
The preparation of this herbal remedy is simple and has been passed down through generations. A typical recipe includes three fingers of turmeric, tamarind soaked in two teaspoons of hot water, two teaspoons of coconut sugar, and three glasses of hot water. The drink is consumed for seven days before menstruation and continued for two days during menstruation [37]. Beyond managing menstrual disorders, this herbal drink is also believed to refresh the body, reduce acne, alleviate digestive issues, and improve blood circulation.
The therapeutic benefits of the turmeric tamarind combination are attributed to the presence of curcumin in turmeric and anthocyanins in tamarind. These bioactive compounds inhibit Cyclooxygenase (COX) enzyme activity, leading to reduced inflammation and decreased uterine contractions, which are associated with menstrual pain [38].
A comparative study by Nadya Fauzia K. et al, (2019) showed that turmeric tamarind juice was more effective in reducing the severity of primary dysmenorrhea compared to ginger drinks [39]. The study employed a quasi-experimental design with a two-group pretest–posttest approach using the Numerical Rating Scale (NRS) to assess pain levels.
Additional studies have supported the efficacy of this herbal combination in alleviating menstrual discomfort [4043]. These clinical findings strengthen the scientific foundation for the use of turmeric tamarind herbal preparations in managing dysmenorrhea.
Cymbopogon nardus (L.) Rendle
C. nardus, commonly known as citronella, has traditionally been used as a mouthwash and a remedy for toothaches and inflamed gums. It has also been employed for its diuretic and analgesic properties, as well as to stimulate urination and menstruation. Although its pain-relieving effects are reported to be less potent than ibuprofen [44] studies have shown that C. nardus possesses significant anti-inflammatory and analgesic potential [45]. In a comparative study, both lemongrass tea and warm water significantly reduced pain levels, as measured by the Numeric Rating Scale (NRS) and Visual Analog Scale (VAS), two hours after consumption [46].
In addition to herbal remedies, many women with dysmenorrhea utilise nonpharmacological strategies. Research shows that methods such as the application of heat and regular physical activity can effectively reduce menstrual pain, with results comparable to those achieved with Nonsteroidal Anti-inflammatory Drugs (NSAIDs) [47]. Heat therapy is believed to work by dilating blood vessels and easing muscle tension, which in turn relieves pain [48]. However, the evidence supporting the effectiveness of dietary supplements (such as vitamins B, D, E, and omega3 fatty acids), as well as alternative therapies like acupuncture, yoga, massage, and various herbal treatments, remains limited and inconclusive.
Among traditional treatments, six medicinal plants are used by hattra practitioners based on empirical knowledge, with pharmacological studies further supporting their analgesic and anti-inflammatory properties.
To preserve and promote this valuable ethnopharmacological heritage, it is crucial to engage younger generations in the practice and study of traditional herbal medicine. Despite occasional perceptions of being outdated, integrating traditional knowledge with modern scientific validation is essential to ensure its continued relevance and its integration into modern healthcare systems.
An analysis of medicinal plants recurrently used in traditional formulations for managing menstrual disorders reveals that Curcuma longa L. is the most prevalently employed species among diverse ethnic communities in Indonesia. From a total of 132 formulations, C. longa appears in 19 instances (14.4%), accounting for 15.4% of the 123 medicinal plant species and is utilized by 23.4% of the 77 documented ethnic groups. Its extensive geographical distribution—from Sumatra to Papua—underscores the widespread cultural recognition and trust in its therapeutic efficacy.
In comparison, Zingiber officinale Roscoe ranks second in 4.9% of the species used. This plant is cited by six ethnic groups located across Java, Kalimantan, and Nusa Tenggara. The application of ginger as a remedy for dysmenorrhea is wellsupported by pharmacological studies highlighting its antiinflammatory and analgesic properties, comparable to Nonsteroidal AntiInflammatory Drugs (NSAIDs).
Other species, including Lawsonia inermis L., Piper betle L., and Tamarindus indica L., each appear in five formulations, contributing approximately 3.8%–4.1% to the total number of medicinal plants and preparations. Although their frequency is lower than C. longa, these plants remain significant due to their distribution among multiple ethnic groups. However, caution is advised for L. inermis as existing pharmacological evidence suggests it may possess abortifacient and antiovulatory activities.
Additional plants with slightly lower usage frequency (3.0%), such as Andrographis paniculata, Cymbopogon nardus, and Graptophyllum pictum, also demonstrate relevance. These species are employed by various ethnic groups in Java, Sulawesi, Nusa Tenggara, and Papua, indicating local variations in ethnomedical approaches to menstrual disorders. Overall, the distribution patterns observed suggest that the use of these medicinal plants for dysmenorrhea is shaped not only by their availability but also by the intergenerational transmission of ethnobotanical knowledge. The prominent use of Curcuma longa reinforces its potential as a leading candidate for the development of hytopharmaceutical products or for incorporation into evidence based complementary medical systems.
Dysmenorrhea remains one of the most common menstrual complaints among women of reproductive age and is known to adversely affect daily functioning and wellbeing. Within Indonesia’s traditional medicine systems, a wide array of plant-based remedies has been employed to address menstrual pain, with C. longa being one of the most prominent choices among traditional healers (hattra).
From both ethnobotanical and pharmacological perspectives, C. longa demonstrates a wide range of bioactivities, including anti-inflammatory, antioxidant, analgesic, hepatoprotective, neuroprotective, and antihyperglycemic effects. Its principal bioactive components, curcuminoids, glycosides, terpenoids, and flavonoids, substantiate these traditional uses. Empirical application of C. longa for dysmenorrhea is further corroborated by preclinical and clinical evidence. For instance, studies by Kashani et al. and Fanaei et al. demonstrated that curcumin can significantly reduce menstrual pain and symptoms of Premenstrual Syndrome (PMS), while also enhancing levels of Brain Derived Neurotrophic Factor (BDNF), a key regulator of mood.
Traditionally, C. longa is often combined with Tamarindus indica to prepare “kunyit asam", a herbal drink believed to exert synergistic effects. Tamarind’s antioxidant rich anthocyanins may enhance curcumin’s therapeutic action by increasing its bioavailability and anti-inflammatory potency. Recent findings suggest that cooking turmeric with acidic substances such as vinegar or tamarind may further potentiate its pharmacological effects, particularly under traditional medicine frameworks such as liverQi stagnation in Eastern medical philosophy.
Besides C. longa, Zingiber officinale also plays an important role in phytotherapy for dysmenorrhea. Ginger’s major constituents gingerol and shogaol, exert mechanisms similar to NSAIDs by inhibiting COX1 and COX2 enzymes. Clinical studies have prevalence, contributing 4.5% of the total formulations and confirmed ginger’s effectiveness, demonstrating outcomes comparable to conventional treatments like mefenamic acid or ibuprofen.
Other medicinal plants, including Piper betle, Lawsonia inermis, and Cymbopogon nardus, also provide notable analgesic and anti-inflammatory benefits. P. betle has shown significant antinociceptive effects in preclinical studies, while C. nardus has milder but measurable analgesic effects. Nevertheless, the use of L. inermis warrants caution due to its documented reproductive effects, particularly its abortifacient and antiovulatory potentials.
In conclusion, the ethnomedical use of plants for dysmenorrhea in Indonesia reflects not only a rich cultural heritage but is increasingly supported by scientific evidence. Bridging traditional knowledge with modern pharmacological validation is vital for the development and legitimization of evidence based herbal therapies.
In Indonesia, traditional healers and various ethnic communities commonly use similar medicinal plants to treat menstrual disorders. The integration of traditional knowledge with modern scientific research provides valuable insights into dysmenorrhea and the development of natural therapeutic approaches. Clinical studies, primarily using pre–post intervention designs and measured with the Numeric Rating Scale (NRS) and Visual Analog Scale (VAS), have shown that Curcuma longa, Zingiber officinale, Tamarindus indica, and Cymbopogon nardus exhibit significant potential in relieving menstrual pain.
Highlights
• Traditional knowledge demonstrates the diverse use of medicinal plants for managing dysmenorrhea. Several plants, such as turmeric (Curcuma longa), ginger (Zingiber officinale), tamarind (Tamarindus indica), and citronella (Cymbopogon nardus), have been supported by both in vivo and clinical evidence. Collaboration between traditional practices and modern scientific research holds great potential for developing effective natural therapies for dysmenorrhea.
• The use of medicinal plants for dysmenorrhea in Indonesia reflects a rich cultural heritage and significant therapeutic potential. Scientific evidence supporting their use strengthens the prospects for developing phytopharmaceutical products and evidence based herbal therapies.
Declarations
Acknowledgements: Our deepest gratitude is conveyed to all traditional healers as resource persons and to the Ristoja team of the Indonesian Ministry of Health in 2015 and 2017.
Authors’ contributions: Conceptualisation: Lucie Widowati, Rini Sasantai Handayani; Data curation: Ani Isnawati, Sukmayati Alegantina, Putri Reno Intan; Formal analysis: Lucie Widowati, Delima Delima, Rachmalina Soerachman; Investigation: Slamet Wahyono, Rohmat Mujahid; Methodology: Delima Delima, Slamet Wahyono; Project administration: Sukmayati Alegantina, Putri Reno Intan; Resources: Slamet Wahyono, Lucie Widowati, Rohmat Mujahid; Supervision: Lucie Widowati; Validation: Sukmayati Alegantina; Visualisation: Rohmat Mujahid; Writing–original draft: Lucie Widowati, Rini Sasanti Handayani; Writing–review editing: Lucie Widowati, Putri Reno Intan, Ani Isnawati.
Competing of interests: There are no financial interests or personal relationships that could appear to have influenced the work reported in this paper.
Ethics approval: This article does not require ethical approval as it is a review article.
Funding: There was no financial support for this study.